




Dry Needling of Trigger Points and Myofacial Release of painful muscles
Acute soreness of muscles after prolonged or unaccustomed eccentric muscle contractions can lead to severe and almost debilitating muscle pain. In some cases, due to the chronic nature of the musculoskeletal condition, trigger points developed which not only alter normal movement but also contribute to referred pain in other regions of the body. These can be a result of the biomechanics of the activity undertaken but also as as result of alterations in immune system pertaining to muscles.
We frequently use dry needling in the accompaniment with Real Time Ultrasound to attain improved fascicular gliding of the myofascia. Hereby, reducing muscle pain and improving biomechanical synergistic muscle action. The mechanism of action involves a cascade of events from the release of nitrous oxide and pro- and anti-inflammatory immune substances to the release of endogenous opioids leading to the reduction in pain and muscle spasm. Primarily, this gives the brain a new reference point of relaxation. Combined with massage and joint mobilisations it becomes immediately apparent that joint tissue compression is much relieved by dry needling, allowing the opportunity for passive movement to lubricate the joint. The relaxed state of muscles (which were in spasm) allows the re-education of the appropriate 'timing' and synergies within and between muscles.
Dry Needling has been shown to result in significant improvements of muscular endurance of knee extensors and hip flexion that persisted 4 wk posttreatment as well as a short-term improvement of muscular endurance of knee flexors in the intragroup analysis of soccer players. Compared with placebo, DN showed a significant effect on hip flexion that persisted 4 wk posttreatment. Compared with a nontreatment control, DN also significantly improved maximum force of knee extensors also 4 wk posttreatment. Compared with a nontreatment control, placebo laser combined with water pressure massage resulted in a small but statistically significant improvement of hip flexion range of motion at treatment end and 4 wk posttreatment (Haser et al 2017 Medicine & Science in Sports & Exercise . 49(2):378-383)
Liu et al. (Arch Phys Med Rehabil. 2015;96(5):944–55) systematically reviewed the effect of DN for TrP associated with neck and shoulder pain, showing a specific and significant short- and medium-term effect. Current studies also suggest that DN may be helpful in reducing pain in the upper quarter and craniofacial region (Curr Pain Headache Rep. 2014;18(8):437) and plantar heel region (Phys Ther. 2014;94(8):1083–94).
Shah et al. (Arch Phys Med Rehabil. 2008;89(1):16–23: J Bodyw Mov Ther. 2008;12(4):371–84) found higher concentrations of substance P (SP), calcitonin gene–related peptide (CGRP), bradykinin, 5-hydroxytryptamine/serotonin (5HT), norepinephrine, tumor necrosis factor α (TNF-alpha), and interleukin 1β in myofascial TrP. After DN, SP and calcitonin gene–related peptide concentrations significantly dropped corresponding with less clinical tenderness and pain of TrP. Besides the mechanical tissue stimulus, with a change in the milieu of local inflammatory parameters (Curr Pain Headache Rep. 2012;16(5):407–12), remote reduction of inflammatory neuromediators such as SP may also be responsible for the effect of DN (Biomed Res Int. 2014;2014:982121).
Trigger Point palpation
Trigger point - gluteus medius
Trigger Points : piriformis, gluteus maximus, quadratus lumborum, levator ani
Trigger Point - adductor magnus. Note the anal referral which is common amongst cyclists who use the adductors to power hip extension
Trigger Points : Obturator Internus and pelvic floor
Trigger point - iliopsoas
It should be noted that we treat many other trigger points in other parts of the body besides the ones illustrated.
Biochemistry of trigger points
Jay Shah experienced musculoskeletal pain and was eventually treated with dry needling. He was so ammazed by it's effect, he made it an adjunct of his other research in a separate field. During a presentation at AAOM, by Jay Shah in 2012, discussing neuromusculoskeletal pain and what lessons may be learnt from the myofascia, he described the following results
Effect of Dry Needling
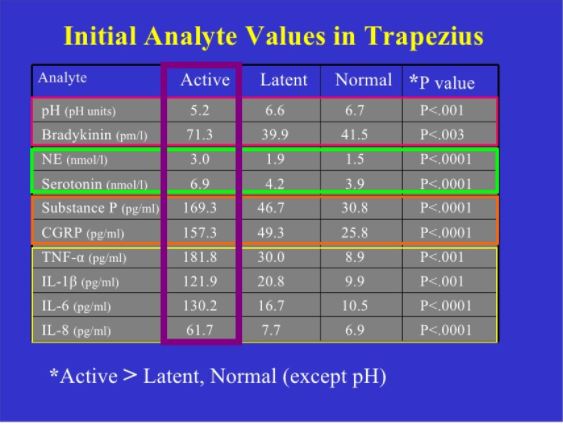
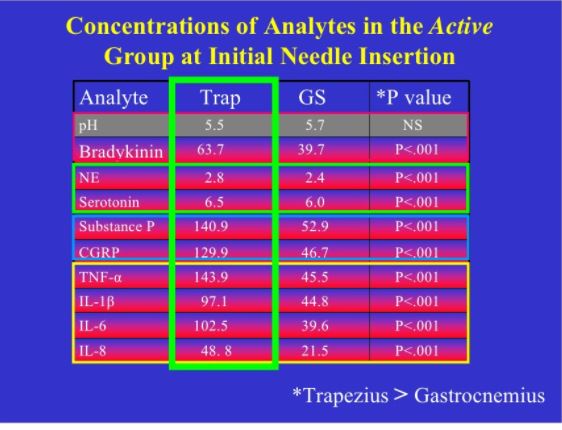
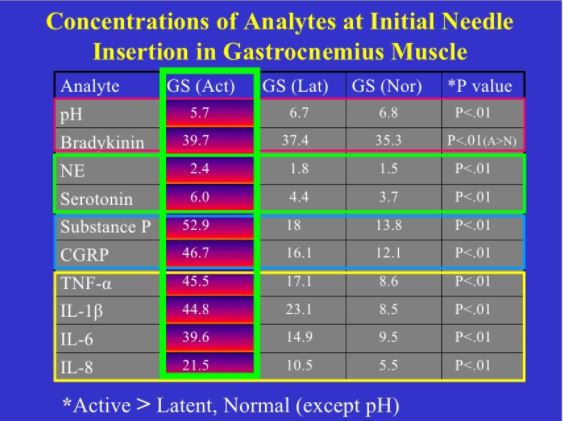
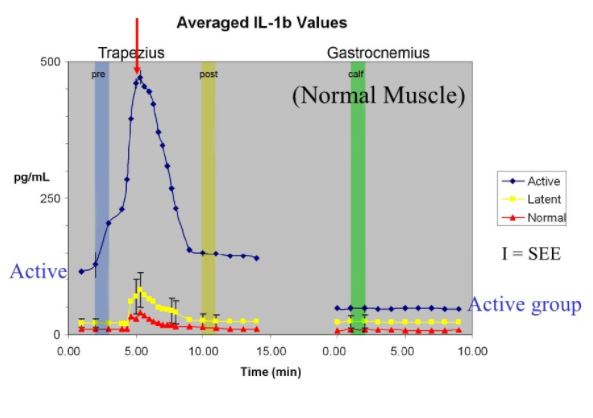
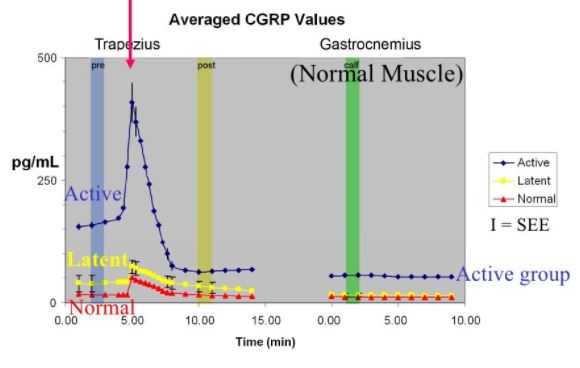
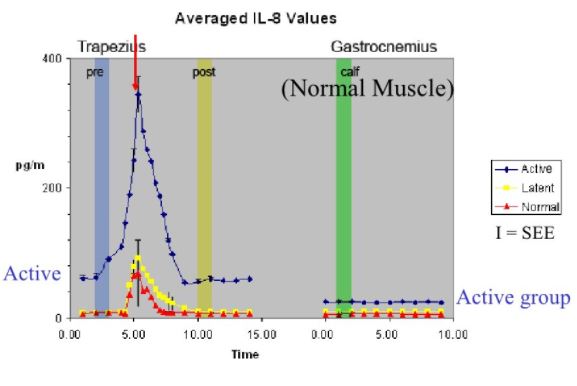
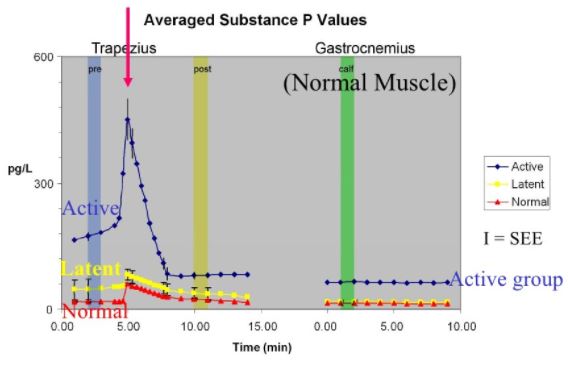
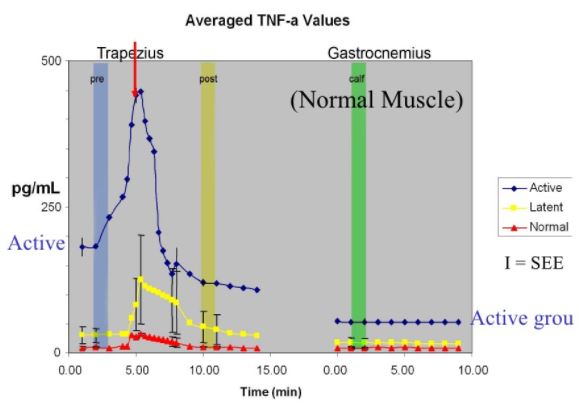
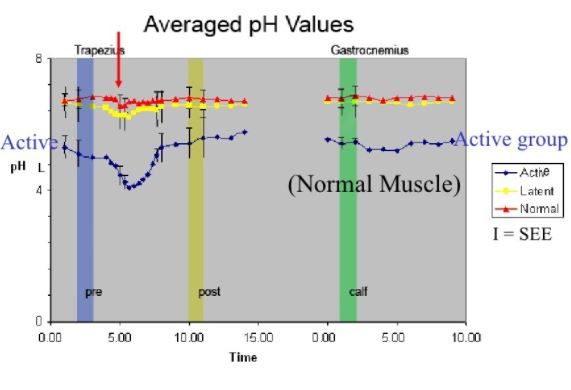
Comparison of normal, latent and active trigger point physiology using microdialysis in the upper trapezius muscle (Shah et al 2005).
These researchers also found similar results for Bradykinin, Calcitonin Gene Related Peptide (CGRP), Substance P, Tumor Necrosis Factor alpha, and Interleukin 1beta. Additionally, reduced pH levels were also seen in areas of active trigger points.
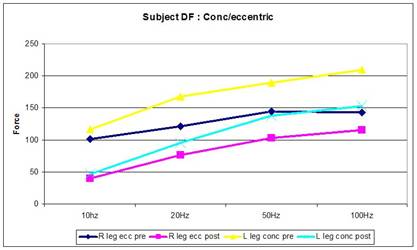
The biomechanics of plyometric (eccentric-concentric) exercise which can give rise to trigger points.
Trigger points have been classically associated with plyometric type of exercise where muscles lengthen during eccentric contraction which although it damages cytoskeletal is considered adaptive in the formation of new sarcomeres. Investigations into eccentric exercise revealed pain 8 hours after initial exercise which was maximal 48 hours later (Newham, Mills, Q uigley, Edwards 1983). These investigators found low frequency fatigue 10 minutes after a 20 minute period of stepping (Newham et al 1983). Additionally, they demonstrated progressive increases in IEMG during the exercise in the rectus femoris (160% increase) and vastus medialis (140% increase) in the eccentric contracting leg (Newham et al 1983). Mechanical damage to the sarcoplasmic reticulum resulting in less calcium release for each excitatory action potential was suggested as the cause of the low frequency fatigue (Newham et al 1983).
However, a number of sites in the myofibrillar complex such as reduce binding sensitivity and capacity of Troponin C for calcium, altered troponin-tropomysosin interaction to impaired binding and force generation by actin and myosin have been implicated in impaired force generation (Green 1990). Indeed, in the absence of any association between relaxation rates and Calcium kinetics raises support for the notion of a rate-limiting process controlling the relaxation of fatigued muscles being located in the contractile proteins (Hill et al 2001). During fatigue the relaxation times can be prolonged as much as 50% (Bigland-Ritchie et al 1986) thus resulting in increased force generation during submaximal stimulation due to tetanic fusion despite a substantial fall in the maximum tetanic force (Bigland-Ritchie et al 1986).
The initial overall loss of force production seen may be due to Desmin and Titan damage (Lieber & Friden 2002). Desmin acts as an extra-sarcomeric mechanical stabilizer between adjacent Z discs and the attachment to the costomere at the sarcolemma (Lieber, Shah & Fridén 2002). The costomere complex contains Talin, Vinculin & Dystrophin which attach to the trans-sarcolemmal proteins Integrin and Dystrophin associated proteins. These proteins allow the lateral transmission of force from actin to the basal lamina containing type IV collagen which is contiguous with the endomysium (Kovanen 2002). Desmin loss after eccentric exercise can occur within 5 minutes, possibly as a result of increased intracellular Calcium leading to Calpain activation and selective hydrolysis of intermediate filament network (Lieber & Fridén 2002). This may result in the ‘popping of sarcomeres' of different length thereby potentially loosing their myofilament overlap of actin and myosin (Lieber & Fridén 2002). Hence, reduced force production would be expected. Additionally, the release of matrix metalloproteinase (MMP) which may degrade the extramyocellular type IV collagen (Korskinen, Kovanen, Komulainen et al 1996). However, this effect occurs many days after exercise (Korskinen et al 1996) and could even effect torque production 28 days after exercise (Lieber & Fridén 2002). This has significant implications in exercise training prescription.
flash file created by Martin Krause 2003
Titan molecules span the gap between the ends of the thick filaments and Z-bands. At the 2007 MPA conference in Cairns, Rob Herbert, provided the AJP oration whereby he explained the significance of Titan as a major determinant of extensibility in muscle fibres. Additionally, he stated that Titan is differentially expressed in human skeletal muscle as short stiff fibres and long compliant fibres.
- Costomeres are 15 different proteins
- Low oxidative muscles have a tendency to tear during eccentric exercise
- Loss of desmin proceeds loss of fibronectin membrane
- Fibre strain results in increased intracellular and extracellular calcium which ?may lead to desmin hydrolysis through calpaine?
- Sarcomere shortening occurs to the detriment of tendon lengthening
- Excitation-contractile coupling may be the area disrupted rather than pure sarcomere disruption
- Structural changes of the disruption of the cytoskeleton include dystrophin (sublaminal membrane protein), sometimes desmin and titin, whereas alpha actin is always OK ?suggesting that calpaine is not the enzyme responsible for protein dysruption?
- Creatine Kinase has no correlation with these cytoskeletal changes
- Inflammatory process important for tissue cleaning and remodelling
- Mechanism for muscle adaptation may be myosin gene regulation - heavy chain myosin isoform upregulation
- Oxygen into the Mitochondria and through the electron transfer chain (ETC) results in ATP use of 20% for power and 80% for heat, therefore people producing less heat may be producing more power?
- Slow twitch muscle fibre concentration varies with the years of training
- Cycling cadence velocity at peak efficiency for slow twitch muscle fibres is 80rpm
Fibroblasts and Loose Connective Tissue
At the APA conference in Sydney during October 2009, Dr Helene Longevin presented her research into the effects of stretching subcutaneous tissue. Superficial and deep fascia are composed of loose and dense connective tissue layers. The loose layers allow dense layers to glide past one another. This tissue contains abundant fibroblasts, immune cells and neurovascular bundles. A 20% static stretch of loose connective tissue for 30minutes significantly increases the size of fibroblasts in vivo and in vitro. Although this mechanism remains unclear it is hypothesised to be due to microtubule reorganisation (Beta-tubulin). Inhibition of growth kinase and Roc prevents the cells from spreading out. Actine polymerisation occurs at the leading edge. Fibro-attraction occurs whereby fibroblasts push forward at it's front edge, whilst retracting the rear (through Rho). Both Rac and Rho are activated simultaneously. The fibroblasts microtubule assembly contributes to connective tissue (C.T) relaxation, which means that tense in connective tissue is actively regulated. Viscoelastic response of loose connective tissue is influenced by specific cytoskeletal inhibitors. Rac increases the equilibrium force. Active C.T tensioin regulation may occur normally in response to sustained chnages in tissue length (e.g. hift in body position). This role may be to prevent sustained mechanical stimulation of other cells within the C.T (immune cells, nerve fibres, blood vessels).
The dense C.T fibroblasts don't respond to stretch due to the stiff matrix preventing the fibroblasts from receiving any strain. Scarring due to injury causes an increase in dense C.T which can be pevented by 10minutes, 2 times per day for 1 week in a suspended tail animal model. The combination of reduced movement and inflammation is a recipe for fibrosis. R-T US can be used as feedback during dry needling to observe C.T movement. In people suffering low back pain the fascial layers are less fluid and less differentiated. Additionally, people with LBP have hicker perivascular C.T. Involuntary muscle spasms may decrease the relative C.T motion during passive movement. Conversely, increased C.T thickness, stiffness and/or viscosity may affect the passive stiffness and range of movement of adjacent muscles.
Intrinsic tension within C.T will have profound effects in the cells within it such as blood vessel precursors stimulating angiogenesis. Similarly, immune cells may be affected by this tension. High amplitude or repetitive tissue stretch may cause injury but can also increase C.T strength. Low amplitude stretch within or slightly beyond the usual ROM may help maintain appropriate mibility and dynamic tissue response. Hence this may represent strong evidence for STM, dry needling, joint mobilisations, muscle energy technqiues, strain-counterstrain techniques and training with Whole Body Vibration.
Additionally, myofascial release techniques and Kinesiotaping can also be employed in order to restore optimal movement function.
Publications into trigger point therapy include
- Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Shah JP et al (2008) Arch Phys Med Rehabil, 89, 16 -23.
- Integrated Dry Needling with new concepts of myofascial pain, muscle physiology and sensitization. Shah JP In : Contemporary Pain Medicine, Integrative Pain Medicine, The Science and Practice of Complementary nd Alternative Medicine in Pain Management. Ed Audette & Bailey, Human Press, Totowa, NJ
- An explanation of Simons' integrated hypothesis of trigger point formation. Gerwin RD, Doomerholt J, Shah JP (2004). Current Pain and Headache reports, 8, 468-475
- Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome. Shah JA & Gilliams EA (2008). J of Bodywork and Movement Therapies, 12, 371-384
- An in-vivo microanalytial technique for measuring the local biochemical milieu of human skeletal muscle. Shah JP et al (2005) J Appl Physiol, 99, 1977-1984
Updated : 1 November 2021
 What We do
What We do What We Treat
What We Treat



















































































































